Post-Injury Rehabilitation
In recent years, many professional athletes have unfortunately faced this type of injury. In basketball, players such as Danilo Gallinari, Derrick Rose, Zach LaVine, and Sergio Llull; in football, athletes like Lorenzo Insigne, Claudio Marchisio, and Nicolò Zaniolo. These are just a few names, but sadly the list of players who have suffered this knee injury is much longer.What is the Anterior Cruciate Ligament (ACL) and why is it so important for the knee?
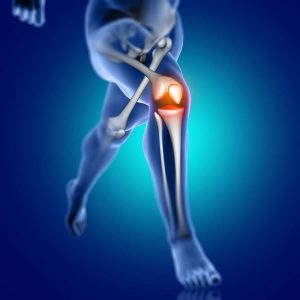
The Anterior Cruciate Ligament (ACL) is a dense band of connective tissue composed of two bundles: the anteromedial (AM) and the posterolateral (PL). It extends from the anterior area of the tibial plateau to the postero-medial portion of the lateral femoral condyle. Typically, this ligament measures between 31 and 38 mm in length and 10 to 12 mm in width. It plays a crucial role in stabilizing the knee joint: it limits the anterior translation of the tibia relative to the femur and also contributes to controlling the internal and external rotation of the knee. Usually, ACL injuries occur without direct contact to the knee joint. The most common mechanism involves non-contact situations such as landing from a jump, sudden changes of direction, or deceleration movements. More specifically, the typical injury pattern is a valgus knee position combined with internal rotation of the tibia relative to the femur—as illustrated in the image below. Injury 1")
In recent years, there has been a noticeable increase in the incidence of this type of injury. This is likely linked both to the way the game is played today (athletes being faster, stronger, and more explosive than in the past) and, above all, to the high workload athletes are subjected to (more training sessions, more matches, and insufficient recovery time).
Statistically, women are more prone to non-contact ACL injuries compared to men, due to anatomical, biomechanical, and hormonal factors.
In general, the main risk factors for this type of injury include:
- Weakness in the core muscles, hip abductors, quadriceps, and hamstrings;
- Stiff landing mechanics;
- Accumulated fatigue and inadequate recovery;
- Knee valgus movements (although recent scientific literature tends to consider these as natural lower limb movements in game situations, rather than a true risk factor);
- Non-modifiable anatomical factors, such as tibial plateau depth, intercondylar notch width, and tibial slope.
What to do in case of a knee sprain or trauma?
- The first crucial step is to go to the emergency room, where an X-ray is usually performed to rule out fractures or bone lesions. When meniscal or ligament involvement is suspected, the patient often reports hearing a “popping sound” at the time of injury, accompanied by severe pain, joint swelling, a feeling of instability, and reduced mobility of the knee.
- If the X-ray is negative but meniscal or ligament damage is still suspected, the patient should be referred to an orthopedic specialist. The orthopedist will typically perform clinical tests such as the drawer test, Lachman test, and Pivot Shift test to assess ACL integrity. If suspicion remains, an MRI is ordered, which remains the gold standard for diagnosing both ligament and meniscal injuries.
- Once an ACL tear is confirmed, the orthopedist and patient will decide together on the most appropriate course of action based on the patient’s individual needs.
Don’t worry—surgery is not the only option. It is entirely possible to live a healthy, active life even with a torn ACL.
Recent scientific literature divides patients with ACL injuries into two main categories:
- COPER patient: patients who do not experience knee instability or giving way and can return to sports without surgery;
- NON-COPER patient: patients who do experience instability and knee giving way, making it impossible to return to pre-injury activity levels without surgery.
And you may ask: “How do I know if I’m a COPER or NON-COPER?”
First, our advice is not to rush into surgery. Waiting two to three months after the traumatic event allows the joint to deflate, mobility to recover, and—most importantly—to begin a pre-operative physiotherapy program focused on strengthening the muscles. The stronger your muscles are before surgery, the better your recovery will be.
Additionally, this prehab phase makes it possible to perform specific strength and functional tests that help both the clinician and the patient determine whether surgery is necessary. This choice should also consider the patient’s age, type of sports activity, and the presence of associated injuries that could further compromise joint stability in the medium to long term.
This approach is known as “Shared decision making”—a process where doctor and patient (or any healthcare professional and their patient) decide together on the best course of action. Patients are, and always will be, active participants in every step of rehabilitation.
Stay tuned for our next article, where we’ll explore the different types of ACL reconstruction surgery and the key stages of rehabilitation.